General Pediatric Dentistry Topics:

Should I Schedule My Child With a Pediatric Dentist or a General Dentist? What’s the Difference?
A pediatric dentist, like Dr. John J. Riehs, is required to complete an additional two year residency (specialty training) in pediatric dentistry beyond dental school. During residency, pediatric dentists receive advanced training in behavior management, child psychology, growth and development, hospital dentistry, interceptive orthodontics, sedation, special needs patients, and techniques to alleviate anxiety and build trust with children and their parents. This extensive training provides pediatric dentists the knowledge and skills to provide a positive dental experience and to educate children on the importance of maintaining good oral hygiene. Furthermore, pediatric dentists limit their practice to treating the oral health needs of Infants and children through adolescence. Because their practice is exclusive to kids, the environment is commonly conducive to children’s appeals.
Why Are Primary Teeth So Important?
Primary teeth are very important because they can still get cavities if neglected. These cavities can affect developing permanent teeth. Primary teeth (baby teeth) are important because:
While the front 4 teeth last until 6-7 years of age, the back teeth (cuspids and molars) aren’t replaced until age 10-13.
Eruption of Your Child’s Teeth
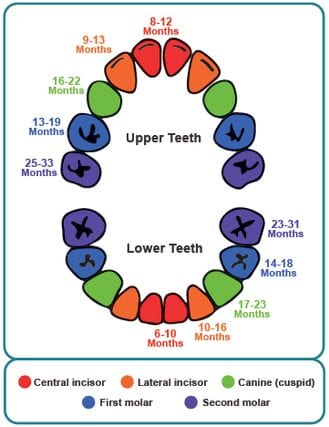
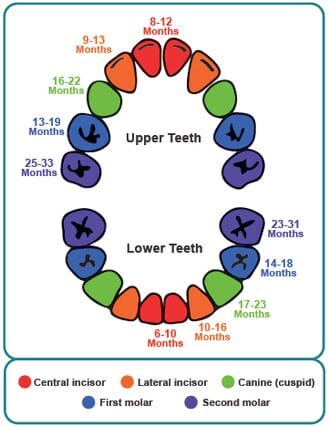
Children’s teeth are forming before birth. As early as 4 months of age, the first baby teeth begin to erupt through the gums. These are the lower central incisors, followed closely by the upper central incisors. All 20 primary teeth should usually appear by age 3, but the pace and order of their eruption varies, depending on the child.
Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors. This process continues until approximately age 21 years of age. Adults can have 28 permanent teeth, or up to 32 including the third molars (or wisdom teeth), depending on their history (teeth extraction/ trauma etc.).
Why Are Primary Teeth So Important?
Primary teeth are very important because they can still get cavities if neglected. These cavities can affect developing permanent teeth. Primary teeth (baby teeth) are important because:
While the front 4 teeth last until 6-7 years of age, the back teeth (cuspids and molars) aren’t replaced until age 10-13.
Eruption of Your Child’s Teeth
Children’s teeth are forming before birth. As early as 4 months of age, the first baby teeth begin to erupt through the gums. These are the lower central incisors, followed closely by the upper central incisors. All 20 primary teeth should usually appear by age 3, but the pace and order of their eruption varies, depending on the child.
Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors. This process continues until approximately age 21 years of age. Adults can have 28 permanent teeth, or up to 32 including the third molars (or wisdom teeth), depending on their history (teeth extraction/ trauma etc.).
Dental Emergencies Can Include:
Dental Radiographs (X-rays)
Radiographs (x-rays) are an important and necessary part of your child’s dental diagnostic process. Without x-rays certain dental conditions will be missed. X-rays can detect much more than cavities. X-rays are often needed to discover erupting teeth, diagnose bone diseases, evaluate injuries and/or plan orthodontic treatment if necessary.
Radiographs also allow dentists to diagnose and treat health conditions that cannot be detected during a clinical exam. If dental problems are found and treated early, dental care is more comfortable for your child and more affordable for you creating a better experience for everyone.
The American Academy of Pediatric Dentistry recommends x-rays and dental exams every six months for children with a high risk of tooth decay. On average, most pediatric dentists request x-rays once. Furthermore, every 3 years, it is a good idea to obtain a panoramic x-ray to view developing teeth and bones.
We are always particularly careful to minimize the exposure of our patients to radiation. However, with modern technology and safeguards, you can rest assured that the amount of radiation received in a dental radiograph/examination is minimal. The risk of dental x-rays are negligible, and often represent a far smaller risk than an undetected and untreated dental problem. We utilize lead body aprons to help protect your child. Today’s equipment filters out unnecessary x-rays and restricts the x-ray beam to the area of interest. High-speed film and proper shielding assure that your child receives a minimal amount of radiation exposure.
Tooth Brushing
Tooth brushingis the most important thing your child will learn for good oral health. However, many toothpastes & polishes can damage teeth or cause harm. Primarily, many contain harsh abrasives, which can wear away young tooth enamel. You should select toothpaste for your child that has been recommended by the American Dental Association and is age appropriate as shown on the box and tube.
It is important to teach children that they should spit out toothpaste to avoid ingesting too much fluoride. Consumption of too much fluoride can result in a condition known as fluorosis.
If your child is too young or unable to spit out toothpaste, consider using less than a “pea size” amount of toothpaste.

Does Your Little One Grind His or Her Teeth at Night?
The nighttime grinding of teeth (bruxism) can be very alarming. Typically, the parent will hear the noise created by the child grinding their teeth during sleep. In addition, one might notice wear (teeth getting shorter).
So what causes bruxism? One suggestion is psychological, and that different types of stress (due to a new environment, divorce, changes at school; etc.) can influence a child to grind their teeth. Another theory pertains to pressure in the inner ear. If pressure changes (i.e. an airplane during take-off and landing — people chewing gum to equalize pressure), it is often a natural response to grind by moving the jaw to relieve this pressure.
Most cases of pediatric bruxism do not require any treatment at all. If we see excessive wear of the teeth (also known as attrition), then we might prescribe a mouth guard (night guard). There are some things to consider (negative) before moving forward with a mouth guard for your child. Firstly, there is a possibility of choking if the appliance becomes dislodged during sleep. Secondly, it could interfere with growth of the jaws. The positive is obvious by preventing wear. We will discuss all the pros and cons of any treatment we deem necessary for your child, and give you the information you need to make an informed decision.
Most children outgrow bruxism, without any treatment necessary. The grinding decreases between the ages 6-9 and children tend to stop completely between ages 9-12.
Thumb Sucking & Pacifier Use
Babies are born with several natural reflexes, including the sucking reflex. It’s a natural reflex, and most infants/children will suck their thumb, finger, or pacifier. The sucking reflex often creates a sense of calm in babies and young children, and helps them to relax and self-soothe. It often leads to a nap or deep sleep.
However, sucking one’s thumb or pacifier beyond the eruption of the permanent teeth can cause serious growth problems in the mouth and with tooth alignment. The intensity of the sucking motion will determine whether or not a dental problem will result. We know that children who just rest their thumbs passively in their mouths (as a habit of placement) with the sucking reflex are less likely to have difficulty than those who vigorously suck their thumbs or a pacifier.
Children should cease thumb sucking and/or pacifier use by the time their permanent front teeth are ready to erupt, typically between the ages of four and six. If allowed to persist into elementary school, peer pressure causes many school-aged children to stop.
A few suggestions to help your child lose the pacifier or stop sucking their thumb:
Use positive reinforcement – praise your child when they refrain from sucking.
Reward your child when he/she refrains from sucking during especially difficult periods (sickness, separation, and times of discomfort).
Work on identifying and relieving causes of anxiety that cause this habit
Provide extra comfort and support for your child, and help them to stay busy and interested in other things.
Dr. Riehs can work with your child to encourage them to stop sucking by explain the consequences.
Remind the children of their habit by bandaging the thumb or putting a sock on the hand at night. Your pediatric dentist may also suggest use of a mouth appliance.
Pulp
The "Pulp" is the center core of the tooth. This area contains primarily nerves and blood vessels. When there has been a severe cavity or trauma to the teeth, there is damage to the pulp area and risk of losing the tooth. In pediatric dentistry we use pulp therapy to maintain the “life” of the affected tooth (in the effort to not lose the tooth entirely). It is often referred to as “nerve treatment,” “children’s root canal,” “pulpectomy,” or “pulpotomy”. The two common forms of pulp therapy in children’s teeth are the pulpotomy and pulpectomy.
Pulpotomy is a process that removes the diseased pulp tissue within the crown portion of the tooth. After the diseased portion is removed, medications and sedative fillings are placed to prevent bacterial growth and calm the remaining nerve tissue. This is followed by a final restoration, usually a stainless steel crown.
Pulpectomy is required when the entire pulp is involved within the crown and root portion of the tooth. This treatment differs in that the diseased pulp tissue is completely removed from both the crown and the root. The canals are cleaned and filled and a final restoration is placed, usually a stainless steel crown.
What Is the Best Timing for Orthodontic Treatment?
Crooked teeth or “malocclusions” can be recognized as early as 2-3 years of age. However, they are most commonly treated when the permanent teeth erupt.
Stage I – Early Treatment – 2 to 6 years: At this young age, we are concerned with underdeveloped dental arches, the premature loss of primary teeth, and harmful habits such as finger or thumb sucking. Treatment initiated in this stage of development is often very successful and many times, though not always, can eliminate the need for future orthodontic/orthopedic treatment.
Stage II – Mixed Dentition – 6-12 years: During this time, we monitor the eruption of the permanent incisors (front teeth) and 6-year molars. Treatment concerns deal with jaw positions and dental alignment problems. This is an excellent stage to start treatment, when indicated, as your child’s hard and soft tissues are usually very responsive to orthodontic and orthopedic forces.
Stage III – Adolescent Dentition – teenage years: This stage deals with the permanent teeth and the development of the final bite relationship.
Prevention:
Begin teaching daily brushing habits as the first tooth appears.
According to the American Academy of Pediatric Dentistry (AAPD), parents should use no more than a smear or rice-size amount of fluoridated toothpaste for children less than three years of age to decrease the risk of fluorosis. Using no more than a pea-size amount of fluoridated toothpaste is appropriate for children aged three to six.
By age 4 or 5, children will be able to brush their own teeth twice a day with supervision and begin working on spitting. Certainly, each child is different, and Dr. Riehs can help you determine whether the child is brushing properly.
When done properly, brushing removes plaque from the inner and outer parts of the teeth, and the chewing surfaces. When teaching children to brush, place the toothbrush at a 45 degree angle; start along gum line with a soft bristle brush in a gentle circular motion. Brush the outer surfaces of each tooth, upper and lower. Repeat the same method on the inside surfaces and chewing surfaces of all the teeth. Finish by brushing the tongue to help freshen breath and remove bacteria.
Flossing is also a great habit to begin. It removes plaque between the teeth, where a toothbrush cannot reach. Flossing should begin when any two teeth touch. You should floss the child’s teeth for them, until they are old enough to do it alone.
Healthy eating habits offer a world of benefits for your well-being – including healthy teeth! Like the rest of the body, the teeth, bones and the soft tissues of the mouth need a well-balanced diet. These days, popular snacks that children eat (fruit snacks, granola bars, candy) can lead to cavities and other dental problems. How long food remains in the mouth also plays a role in the level of decay. For example, hard candy and breath mints stay in the mouth a long time, which cause longer acid attacks on tooth enamel.
If your child must snack (and eating anytime), try to select those nutritious foods from the five food groups, such as low-fat dairy, fresh and cooked vegetables, meats and whole grains – all are healthy alternatives to high-sugar grazing.
How to Prevent Cavities
Brushing your teeth twice daily helps to remove bacteria and the food particles left over from eating that can create cavities. For babies, use a wet gauze or clean washcloth to wipe the plaque from teeth and gums. Avoid ‘propping the bottle’ or putting your child to bed with a bottle filled with anything other than water.
Diet plays a role as well (as mentioned above) so it’s always a good idea to try and limit sugar. Especially hard candies and mints – things that stay in the mouth for a while and have a solid amount of time to begin their attack on your child’s teeth.
Our office might also suggest protective sealants or home fluoride treatments for your child. Sealants can be applied to your child’s molars to prevent decay on hard to clean surfaces.
Healthy eating habits offer a world of benefits for your well-being – including healthy teeth! Like the rest of the body, the teeth, bones and the soft tissues of the mouth need a well-balanced diet. These days, popular snacks that children eat (fruit snacks, granola bars, candy) can lead to cavities and other dental problems. How long food remains in the mouth also plays a role in the level of decay. For example, hard candy and breath mints stay in the mouth a long time, which cause longer acid attacks on tooth enamel.
If your child must snack (and eating anytime), try to select those nutritious foods from the five food groups, such as low-fat dairy, fresh and cooked vegetables, meats and whole grains – all are healthy alternatives to high-sugar grazing.
How to Prevent Cavities
Brushing your teeth twice daily helps to remove bacteria and the food particles left over from eating that can create cavities. For babies, use a wet gauze or clean washcloth to wipe the plaque from teeth and gums. Avoid ‘propping the bottle’ or putting your child to bed with a bottle filled with anything other than water.
Diet plays a role as well (as mentioned above) so it’s always a good idea to try and limit sugar. Especially hard candies and mints – things that stay in the mouth for a while and have a solid amount of time to begin their attack on your child’s teeth.
Our office might also suggest protective sealants or home fluoride treatments for your child. Sealants can be applied to your child’s molars to prevent decay on hard to clean surfaces.
What Are Sealants?
Sealants are protective coatings placed on the biting surfaces of molar (primary and permanent) teeth to prevent cavities. Sealants act as a shield for the tooth protecting it from food, plaque, bacteria, and acids that in combination cause cavities. According to research transmitted by the American Academy of Pediatric Dentistry (AAPD), sealants reduce the risk of cavity formation by 67%. Investing in early prevention decreases future costs associated with fillings and/or crowns.
How Are Sealants Applied?
- Plaque and food debris is removed from the tooth.
- A blue etching gel is placing on the tooth surface and allowed to remain for less than half a minute.
- The etching gel is rinsed away with water and the tooth is dried.
- A thin layer of liquid sealant (plastic) material is flowed onto the top surface of the tooth.
- A light is placed over the sealant which hardens the sealant (plastic) material.
How Long Do Sealants Last?
Research shows sealants last for many years. Therefore, your child should be protected throughout most of his/her adolescence. By avoiding biting hard objects and focusing on proper hygiene, sealants will last even longer. If, however, a sealant breaks down, it can be easily replaced.
Fluoride
Fluorideis a compound that contains fluorine, a natural element. Small amounts of fluoride used on a frequent basis helps prevent tooth decay. In areas where fluoride does not occur naturally, it may be added to community water supplies. Research shows community water fluoridation has lowered decay rates by over 50%, which means that fewer children grow up with cavities. Fluoride can be found as an active ingredient in many dental products such as toothpaste, mouth rinses, gels and varnish.
How Does Fluoride Work?
Fluoride inhibits loss of minerals from tooth enamel and promotes remineralization (strengthens weak areas of enamel and initial stages of cavities). Fluoride also inhibits bacterial growth which prevents acid production of the bacteria that causes cavities. Risk for decay is further reduced when fluoride is used in combination with a healthy diet and proper dental hygiene.
Is Fluoride Safe?
Using fluoride for the prevention and control of decay is proven to be both safe and effective. In optimal amounts, it extremely effective in strengthening enamel. In excess doses, fluoride can cause a condition called fluorosis. Fluorosis is usually mild with white specks on the teeth that are unnoticeable. In severe cases of fluorosis, the enamel may be pitted with brown discolorations.
What is Topical Fluoride?
Topical fluoride is a preventive agent applied to tooth enamel at your dental cleaning appointment. It comes in several different forms. A dental gel or foam fluoride is placed in a foam tray and held against the teeth for several minutes, after which the child is advised not to eat or drink for 30 minutes. A fluoride varnish is brushed or painted on the enamel. Patients are able to drink or eat immediately after placement because of the sticky adherence of the fluoride solution. Varnish is especially useful for younger children who may not tolerate a fluoride tray or wish to wait thirty minutes to eat or drink.
Being Aware of a Child’s Potential Sources of Fluoride Can Help Parents Prevent the Possibility of Dental Fluorosis.
Some of these sources are:
Too much fluoridated toothpaste at an early age.
The inappropriate use of fluoride supplements.
Hidden sources of fluoride in the child’s diet.
Two and three year olds may not be able to expectorate (spit out) fluoride-containing toothpaste when brushing. As a result, these youngsters may ingest an excessive amount of fluoride during tooth brushing. Toothpaste ingestion during this critical period of permanent tooth development is the greatest risk factor in the development of fluorosis.
Excessive and inappropriate intake of fluoride supplements may also contribute to fluorosis.
Fluoride supplements including drops and tablets, as well as fluoride fortified vitamins should not be given to infants younger than six months of age. After that time, fluoride supplements should only be given to children upon the recommendation of your pediatrician or pediatric dentist and only after all of the sources of ingested fluoride have been accounted.
Certain foods contain high levels of fluoride, especially powdered concentrate infant formula, soy-based infant formula, infant dry cereals, creamed spinach, and infant chicken products. Please read the label or contact the manufacturer. Some beverages also contain high levels of fluoride, especially decaffeinated teas, white grape juices, and juice drinks manufactured in fluoridated cities.
Sports welcome all sorts of dental emergencies. When your child begins to participate in recreational activities and organized sports, injuries can (and most likely WILL) occur.
A properly fitted mouth guard, or mouth protector, is an important piece of athletic gear that can help protect your child’s pearly-whites, and should be used during any activity that could result in a blow to the face or mouth. Mouth guards help prevent injuries to the lips, jaw, face, tongue and help prevent broken teeth. Don’t worry, a well-fitted mouth guard will be comfortable, and your child will still be able to talk and breathe. Call us or ask Dr. Riehs about custom and store-bought mouth protectors.
Pediatric Dental Sedation Topics:
Nitrous Oxide
Nitrous oxide, commonly called “laughing gas,” is a breathable gas which is commonly used to relieve children’s pain and anxiety during dental procedures. It is a blend of two gases, oxygen and nitrous oxide, which is given through a small breathing mask placed over the child’s nose. The American Academy of Pediatric Dentistry recognizes this technique as safe, effective, and non-addictive. The mixed gas is easily inhaled with normal breathing and is quickly eliminated from the body. Your child remains fully conscious and maintains all protective reflexes.
Considerations Prior to Nitrous Oxide Use:
General Anesthesia
General anesthesiais recommended for very young children, apprehensive children, and children with special needs/or disabilities that would not work well under conscious sedation or with intravenous (I.V.) sedation. General anesthesia is a stronger type of sedation and will result in your child being completely asleep. General Anesthesia would be the same as if he/she was having a standard surgical procedure, such as implementation of ear tubes, tonsil removal or hernia repair.
This is only performed in a hospital or outpatient setting. Certainly, the assumed risks are greater than that of other treatment options. However, please keep in mind that if this type of sedation is suggested for your child by Dr. Riehs, the potential benefits have been deemed to outweigh the risks. Dr. Riehs’ suggestions are carefully thought out, and are in the best interest of the child (depending on that child’s needs) as well as the procedure or treatment prescribed.
Most pediatric medical literature places the risk of a serious reaction in the range of 1 in 25,000 to 1 in 200,000, which is far better than the assumed risk of even driving a car daily. If this type of sedation is recommended, but not chosen, the inherent risks are multiple appointments, potential for physical restraint to complete treatment and possible emotional and/or physical injury to your child in order to complete their dental needs. The risks of NO treatment include tooth pain, swelling, and infection, the spread of new decay, damage to developing adult teeth and possible hospitalization from dental infection.
Preparing for Your Child’s Appointment:
After Care for Appointments Utilizing General Anesthesia:
Early Infant Dental / Oral Care:
Why Are Primary Teeth So Important?
Primary teeth are very important because they can still get cavities if neglected. These cavities can affect developing permanent teeth. Primary teeth (baby teeth) are important because:
While the front 4 teeth last until 6-7 years of age, the back teeth (cuspids and molars) aren’t replaced until age 10-13.
Eruption of Your Child’s Teeth
Children’s teeth are forming before birth. As early as 4 months of age, the first baby teeth begin to erupt through the gums. These are the lower central incisors, followed closely by the upper central incisors. All 20 primary teeth should usually appear by age 3, but the pace and order of their eruption varies, depending on the child.
Permanent teeth begin appearing around age 6, starting with the first molars and lower central incisors. This process continues until approximately age 21 years of age. Adults can have 28 permanent teeth, or up to 32 including the third molars (or wisdom teeth), depending on their history (teeth extraction/ trauma etc.).
One of the most serious causes of tooth decay in pediatric dentistry is continuous sugary liquid exposure to teeth. This is often known as “baby bottle tooth decay”. Among these liquids are milk (including breast milk), formula, juices, Gatorade, and other sweetened drinks.
Putting your baby to bed for a nap or at night with a bottle with anything other than water can lead to rapid tooth decay. This occurs because the high-sugar settles around the child’s teeth giving plaque bacteria an opportunity to flourish and produce acids that attack tooth enamel.
If you must give the baby a bottle to comfort them at night, use water. If your child won’t fall asleep, gradually dilute his usual beverage with water over a period of two to three weeks. After each feeding, you might consider wiping the baby’s gums and teeth with a damp washcloth or gauze pad to remove plaque.
